 Development of ultrasonic guidance
Development of ultrasonic guidance
With the development of Sound Navigation and Ranging (SONAR) technology,ultrasound was first introduced as a medical diagnostic aid after World War II. The physical principle of medical ultrasound imaging is that when a pulse of ultrasound is sent into soft tissue, this pulse interact with the tissue through reflection and refraction at organ boundaries and varying amounts of ultrasound are reflected back to the source according to the difference of acoustic impedance among tissues, which are received and processed by ultrasound machine and consequently display on the screen
[10]. Reported applications of diagnostic ultrasound include diagnosing hemo-pneumothorax
[11], musculoskeletal injuries
[12] and different causes of acute abdominal pain
[13]. Diagnostic ultrasound can meet the need of rapidly diagnosing life-threatening conditions at the bedside
[14], and thus has been widely used in the clinical medicine. Furthermore, its ability to provide real-time image expands its great potential in accurate guidance of catheter localization. Strong evidence indicates that ultrasonic guidance can reduce the incidence of complications and adverse events during cannulation, and meanwhile, improve the successful rates
[15-17]. However, the ultrasound guidance of cannulation also has some limits. On the one hand, both doctor’s skills and patient’s conditions have a great influence on the results of cannulation. A survey from the American Board of Emergency Medicine indicated that the top three perceived barriers to guide central venous catheter placement using ultrasound are insuf?cient training (45%), overtime-consuming (26%), and lack of correct equipment and preferred body site not amenable to ultrasound usage tying for the third (19%)
[18]. Therefore, increasing ultrasound training in emergency department can effectively decrease the rate of unsuccessful cannulation
[19]. In addition, obese patients and patients with subcutaneous emphysema or chronic obstructive pulmonary disease are unsuitable for ultrasonography
[20]. On the other hand, the acoustic impedance of catheter is similar to the acoustic impedance of human tissue, which causes the poor visibility of catheter, so the confirmation of catheter tip position usually needs adept skill and perfect probe angle. Accordingly, a lot of efforts have been made in different fields to increase the accuracy of catheter placement by ultrasound.
Using materials with higher or lower acoustic impedance
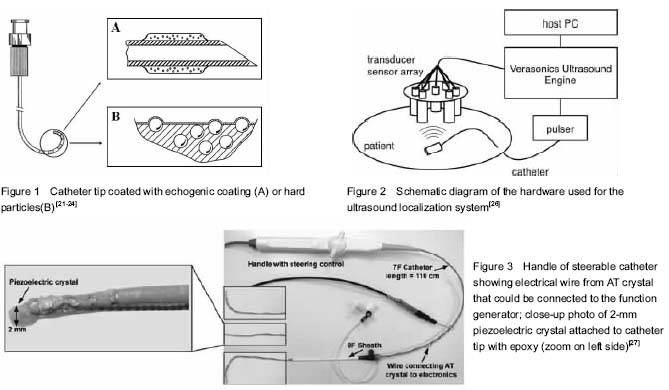
At present, the technique of ultrasound-guided catheter insertion is mature because of the flexible tip guide wire which is withdrawn at the end of puncture, but the confirmation of catheter tip position with ultrasound at the bedside for critically ill patients is still difficult. Since most catheters have similar acoustic impedances to the tissues into which the catheter is inserted, the visibility of catheters is poor that increases the difficulties of accurate placement. Therefore, increasing the differences of acoustic impedances between the catheter materials and tissues can significantly improve the visibility of catheter by ultrasound. Some researchers have tried to enhance ultrasonic images by using echogenic coating. A polymer composite coating contains a plurality of fine gas bubbles (
Figure 1A)
[21]. Echogenic coating provides the catheter with acoustic impedance quite different from that of human tissue and increases ultrasound scattering by a simple, inexpensive and efficient mean of applying a polymer composite coating that has acoustical irregularities
[22]. Other researchers have made a thin interface layer containing hard particles such as metal, metallic oxide or glass to enhance the visibility of catheter
(Figure 1B). Ueshima
et al[24] coated a nerve-stimulating needle with hard microscopic glass beads. Their studies showed that the modified needle provided greater visualization than the non-coated needle at a depth of 2.5 cm on the ultrasound image.
Alternative approaches
Alternative approaches have been developed and focused on enhancing ultrasound equipments or improving ultrasonic guidance system. Kim
et al [25] invented a photoacoustic probe by combining ultrasonic probe with optical fiber: a short laser pulse generates ultrasound by thermo-elastic expansion at biologic tissues where the laser pulse is absorbed, and the ultrasonic waves are finally displayed as a photoacoustic image. The photoacoustic imaging has the superiority of combining high spatial resolution of ultrasonic images with high contrast ratio of optical images.
Mung
et al [26] designed a real-time catheter localization system that can be applied to abdominal aortic aneurysm procedures. They equipped the catheter-tip with a single element ultrasound transducer and the ultrasound pulse transmitted by it was received by an array of seven external single element ultrasound receivers, which were held in the shape of the 20 cm diameter array by a custom made acrylic plate (
Figure 2). The received signals provided time of flight measurements which then provided the location estimate. Water tank validation was tested under three experimental conditions. The first was in a water tank only; the second included a slab of pork belly, mounted beneath the sensor array to simulate the abdominal wall; and the third included an additional nitinol-dacron abdominal aortic aneurysm stent graft. However the result was not as expected, and only the results obtained from the water tank met their initial design goal of < 2 mm root mean square error.
McMahon
et al[27] fitted a small piezoelectric crystal at a steerable catheter tip which could be driven to vibrate by using a function generator (
Figure 3). The physical principle of this system is when a specific frequency interacts with a vibrating surface the reflected ultrasound field has two components at different frequencies. Assuming the ultrasound frequency is f1 and the surface vibration frequency is f2, then the reflected signal will have two frequencies, (f1+f2) and (f1−f2), respectively, which
then is interpreted by the pulsed-wave Doppler mode. The results indicated that after the 10 navigational trials, the average final distance of the catheter tip from the target was (2.4±1.2) mm. Further animal studies also showed high accuracy of ultrasound navigation of this active catheter prototype located inside the beating left ventricle
[28]. However, this new type of catheter still has limitations. The PW Doppler mode identifies the crystal tip, but not the tip of the catheter. The limitation causes several technical obstacles, including the difficulty and problematic logistics of placing the crystal at the tip of the catheter.